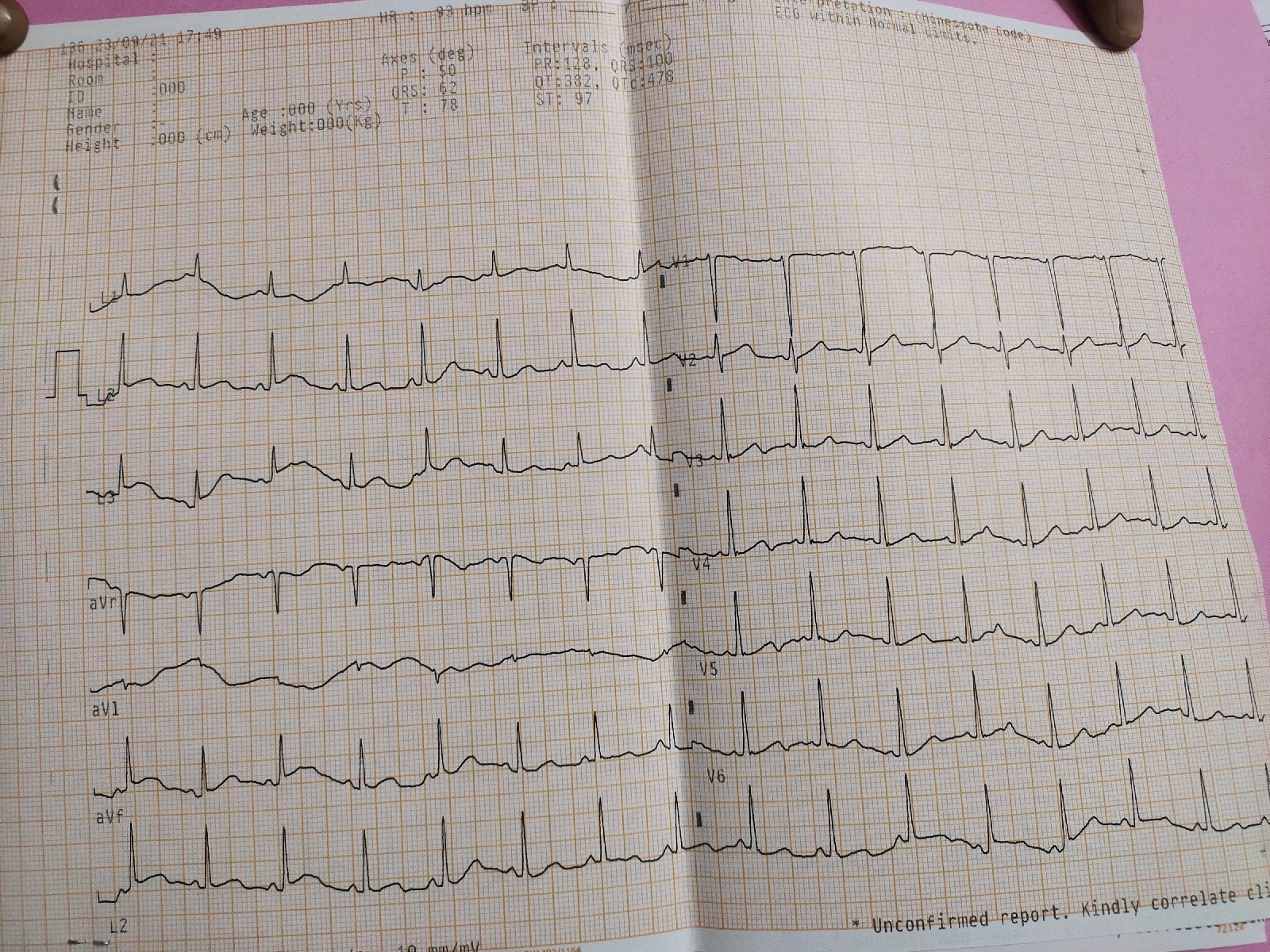
A18 year y female, fever with thrombocytopenia
Unit 1 admission Ward case Dr K VAISHNAVI PGY3 DR NIKITHA PGY3 DR RAVEEN PGY2 A 18 year old female , student presented to the casuality with C/O fever with chills since 10 days H/o nausea present No H/O bleeding manifestions Pt was apparently asymptomatic 10 days back ,later she developed high grade continuous type of fever subsided on medication associated with chills and aggravated since 4 days History of cold present 10 days back subsided on taking medication,diurnal variation absent History of cough with mild scanty sputum ,mucoid in constistency Not associated with giddiness Head ache +,myalgia + Past history : Not a K/C/O DM,HTN,Asthma ,TB,epilepsy No similar complaints in the past Personal history : Diet - mixed Appetite - decreased Sleep - adequate Bowel movements : regular Bladder movements : regular No history of smok...